
If you have struggled with tension or pain in your neck for a long time, there is a high probability that you have tried almost everything. Neck massages. Stretching. Perhaps a chiropractor. Maybe you’ve even been given exercises to do at home that help a little, but the problem always returns.
What I want to tell you in this post is something most people have never heard. And that is that your neck might not be the problem at all.

What I am sharing here is a combination of established anatomy, osteopathic clinical understanding, and my own experience from the treatment table. Not everything is supported by large randomized controlled trials, but it is founded in anatomical connections that make clinical sense. And these are connections I see confirmed again and again with my clients.
The neck is a symptom. Not always the cause.
When I examine clients with neck pain, I don’t just look at the neck. I actually start somewhere else entirely. I start with the breath.
It might sound strange. But there is a direct anatomical connection between your diaphragm, your breathing, and the tension in your neck. And when I explain the mechanics behind it, it suddenly makes perfect sense to most people.
The nerve that connects your diaphragm to your neck
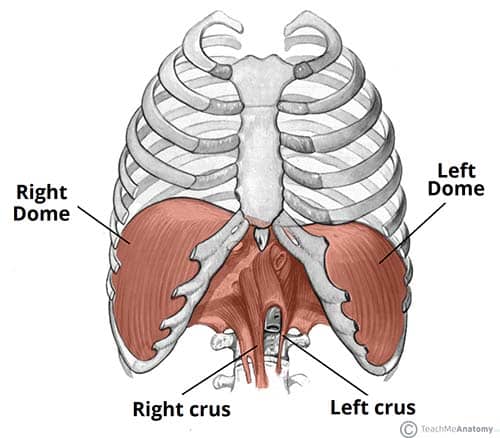
The diaphragm is the large breathing muscle that sits like a dome under the lungs and separates the chest from the abdomen. It is the primary engine behind your breath.
What is interesting here is which nerve controls the diaphragm. It is the phrenic nerve. And it originates from C3, C4, and C5 in the neck—right in the middle of the neck.
This means that the diaphragm and the neck share the same nervous system. The osteopathic understanding is that when the diaphragm is chronically tense and overloaded, it can contribute—via the phrenic nerve—to increased tone and tension in the neck segment it is connected to. It is not the neck itself that is the problem, but a neurological connection that maintains an elevated level of tension.
What I see on the treatment table
In my examination of clients with neck pain, I ask them to turn their head as far as they can to the right and left. Then, I place my hands under the front rib cage and work on inhibiting the diaphragm for a few minutes. And then I ask them to turn their head again.
For many clients, there is a noticeable difference in mobility right then and there. Without me having touched the neck.
This is, of course, a clinical observation and not a diagnostic test with scientifically validated measurements. And the diaphragm is not always the full explanation. The neck is affected by many factors in combination, and the diaphragm is one of them. But when the connection is present, it is a strong indication that the treatment should start with breathing, not locally in the neck.
The story of Oskar, who could see more of the wall
One of my clients, Oskar, came in for osteopathic treatment recently. His wife was in a course of osteopathy with me and had sent him along because she was tired of hearing him complain about the discomfort in his neck. His own words, not mine 🙂
He had office work, and the neck tension had increased over time. It used to be resolved with a few neck movements during the workday. But after being sick for a couple of weeks and returning to the office, the tension was directly bothersome and caused tension headaches.
During the examination, I asked him to turn his head to the right. He moved a fair way but had clearly limited rotation. Then I inhibited his diaphragm under the front rib cage. Then I asked him to turn again.
He said WOW.
Suddenly, he could see significantly more of the wall on the right side. It completely surprised him. And that is exactly the reaction that shows we are on to something right.
In the examination, I also found that his shoulders almost couldn’t drop completely into a resting position. Upon inhalation, they lifted visibly and did not come back down. The scalenes, upper trapezius, and levator scapulae were all massively tense and were taking over the breathing work from a diaphragm that was no longer doing its part.
In the first treatment, we worked with the diaphragm, and he noticed improved neck mobility and less discomfort that very same day. He was given a breathing exercise to take home to start rebuilding the diaphragm’s function and break the pattern of shallow, high-thoracic breathing.
In the subsequent treatments, we continued working on the inhibition of the scalenes and the upper neck and shoulder muscles, joint mobilization of the lower ribs and thorax, and more work with the diaphragm and the structures sitting just below it. The goal was to give the entire system the freedom to breathe deeper and more naturally again.
After three treatments, he was back to his old level. But with one important difference. He had gained a new awareness of his own breathing and worked actively with the exercises. He is now well on his way to becoming completely pain-free.
What happens when breathing becomes shallow?
The short answer: the body finds another way.
The diaphragm is designed to do most of the breathing work. It pulls downward during inhalation, creating negative pressure in the chest and allowing the lungs to fill. When the diaphragm is stiff and restrictive, it is unable to do that work effectively.
So the body recruits help from the accessory respiratory muscles. Muscles that are actually intended to help during high physical strain, not for pumping breath at rest. They are located in the neck and shoulders. The scalenes, sternocleidomastoid, the upper trapezius muscles.
The result is breathing that lives in the upper part of the chest and lifts the shoulders slightly with every breath. You don’t notice it yourself because it happens so gradually. But over time, it creates a chronic overload in the neck and shoulders.
Why does the diaphragm get stiff?
The most common cause is sedentary work combined with little or no movement in the thorax and lower ribs.
The diaphragm, like all other muscles and tissues in the body, depends on movement to maintain its mobility and function. If you sit for many hours a day leaning slightly forward in front of a screen, the lower ribs are compressed, and the diaphragm works within a limited range of motion. Over time, it loses its full excursion and becomes shorter and stiffer.
It is a “use it or lose it” principle. And it particularly affects people who have never done mobility training or movement that consciously opens the chest.
The classic picture I see in my clinic is men in their 50s who have sat at a desk for years and have never thought about their breathing or thorax mobility. They come in with a stiff mid-neck and a closed front of the chest. When I find the diaphragm hypertonic during the examination, it almost always correlates.
“Nursing-neck” is the same problem in another form
Another pattern I see frequently is women who have recently given birth and are struggling with neck pain.
When you hold and breastfeed a baby for many hours a day, the body is constantly leaning slightly forward with your arms in front of your body. This is a position that compresses from the front and leaves very little room to breathe deep down into the lower ribs. The body adapts, and the breathing moves upward, where there is the most space. That is the upper lungs and the shoulders.
The result is the same as with office work. The accessory respiratory muscles in the neck and shoulders gradually take over more of the work, and the neck becomes chronically tense.
The body is just doing what it was designed to do. It finds the easiest path. It’s not “wrong” of the body. But it is worth understanding and working with.
What can you do yourself?
The first and most important thing is to become aware of where your breath lives.
Place your hands on your lower ribs. Are you breathing so that the ribs move outward to the sides and backward? Or are you mostly lifting your shoulders and expanding the top of your chest?
If it is primarily the latter, it is a sign that the accessory respiratory muscles are working more than they need to. You cannot change a breathing pattern overnight. But awareness of it is the first step. And it requires no equipment or time. Only a moment of attention.
When does it make sense to seek help?
If you have had neck pain for a long time and have never looked at the connection to breathing and the diaphragm, it can make a lot of sense to have it properly examined.
In an osteopathic treatment with me, we perform the inhibition test I described earlier, so you can feel for yourself whether the diaphragm plays a role in your neck pain. If it does, we work directly on relaxing the diaphragm and restoring mobility to the thorax and lower ribs. And we test the neck continuously along the way, so you can feel the difference.
There are many other connections between neck tension and the rest of the body. Therefore, I always test you thoroughly, and we adapt the treatment directly to the findings I make in your specific examination!
You are welcome to book an appointment for osteopathic treatment with me at Livets Klinik in Nørrebro. If you are unsure whether it makes sense for your situation, you are always welcome to write to me before you book.
In case of persistent or increasing pain, you should always contact your doctor to rule out other causes.